

NEJM Volume 361:998-1008
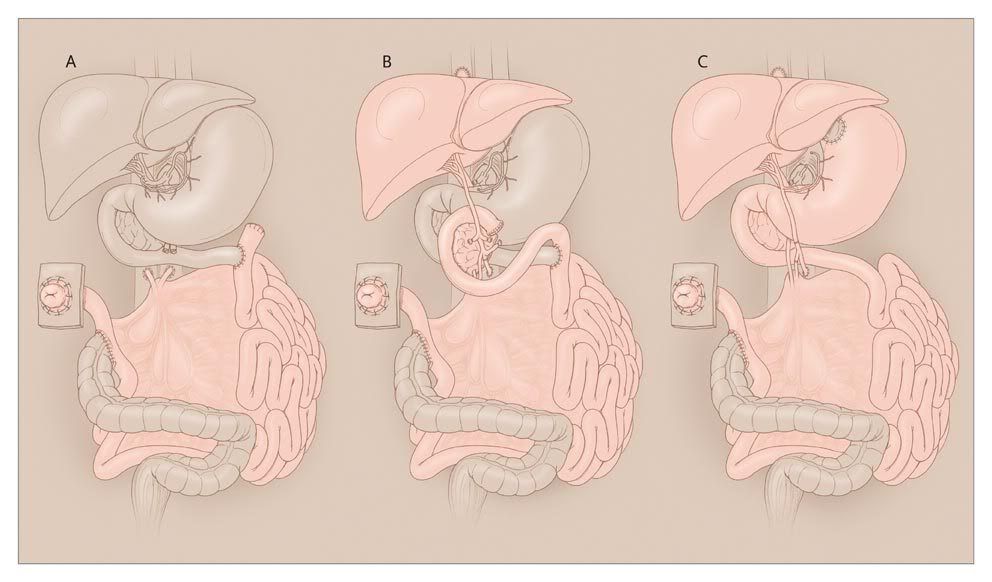
Three Types of Transplants in Intestinal Failure.
When the small intestine (jejunoileum) is transplanted alone, it is referred to as an isolated intestinal transplant (Panel A), with systemic drainage to the vena cava. A composite liver and intestinal transplant usually includes the duodenum and an intact biliary system and portal circulation, with the native foregut preserved (Panel B). In a multivisceral transplant, which involves the liver, stomach, duodenum, pancreas, and small intestine, the foregut is removed and a new stomach is transplanted (Panel C). This type of transplant sometimes includes the colon, kidney, or both. The transplanted organs are shown in pink, and the native organs or structures are shown in light brown.
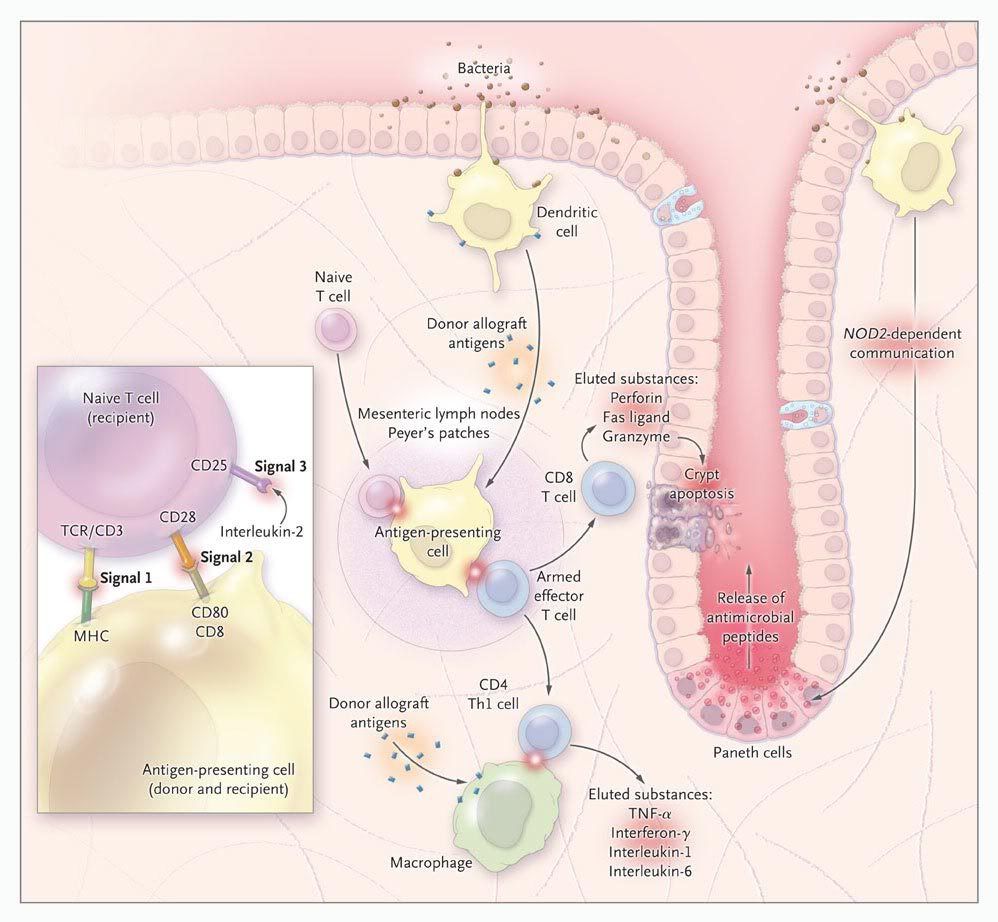
The immunologic response involves six steps, some of which may occur simultaneously. Naive T cells infiltrate the allograft and undergo priming and activation in the donor mesenteric lymph nodes and Peyer's patches. In other solid organs, such priming occurs primarily in recipient lymphoid tissues. Donor antigen-presenting cells, such as dendritic cells, then ingest and display the "foreign" graft antigens in association with class I and II molecules of the major histocompatibility complex (MHC) (see inset). Antigen-presenting cells are stimulated to express costimulatory effectors required to "arm" naive CD8+ cytotoxic T cells and predominantly CD4+ type 1 helper T cells (Th1 cells). The CD8+ cytotoxic T cells attack certain donor-cell targets and produce substances, including perforin, granzyme, and Fas ligand, that lead to crypt-cell apoptosis. Armed Th1 cells provoke an inflammatory state driven by the production of cytokines, including interferon- . The dendritic cell also maintains immune defenses of the epithelium by regulating secretion of the antimicrobial peptide human defensin 5 from Paneth cells by means of NOD2-dependent circuits. Recipients with mutations in the NOD2 gene are at significantly increased risk for immunologic graft loss, possibly owing to inadequate antimicrobial defense, which results in epithelial damage, bacterial invasion, and a secondary inflammatory response. The inset shows the signals involved in the immune response involving the recipient naive T cell and antigen-presenting cells. Tacrolimus interferes with signal 1. To date, no inhibitors to block signal 2 have been approved for use in humans. Interleukin-2 monoclonal antibodies and sirolimus (rapamycin) inhibit signal 3. TCR denotes T-cell receptor, and TNF tumor necrosis factor.
. The dendritic cell also maintains immune defenses of the epithelium by regulating secretion of the antimicrobial peptide human defensin 5 from Paneth cells by means of NOD2-dependent circuits. Recipients with mutations in the NOD2 gene are at significantly increased risk for immunologic graft loss, possibly owing to inadequate antimicrobial defense, which results in epithelial damage, bacterial invasion, and a secondary inflammatory response. The inset shows the signals involved in the immune response involving the recipient naive T cell and antigen-presenting cells. Tacrolimus interferes with signal 1. To date, no inhibitors to block signal 2 have been approved for use in humans. Interleukin-2 monoclonal antibodies and sirolimus (rapamycin) inhibit signal 3. TCR denotes T-cell receptor, and TNF tumor necrosis factor.


 留言列表
留言列表
 線上藥物查詢
線上藥物查詢 